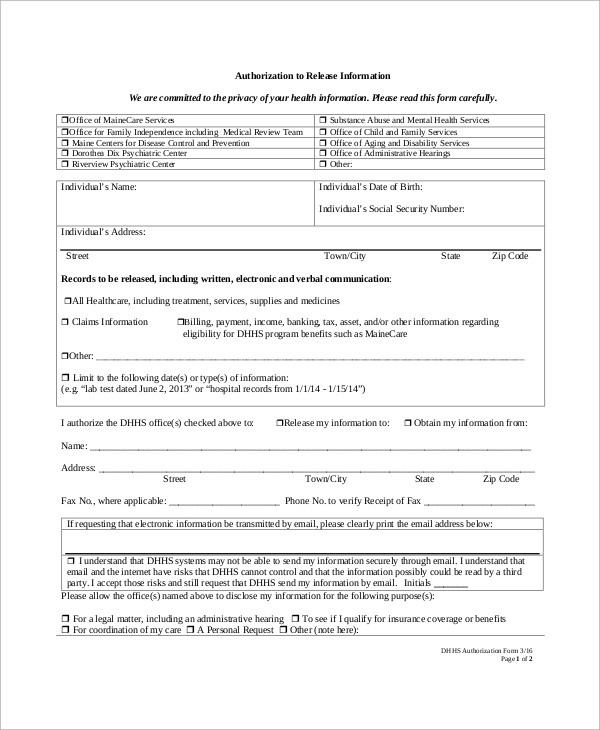
Authorization Authorization For Release Of Health Information Health Information Release Authorization For Release Of Health Information pedalitabuayale Saturday, October 17, 2020 Authorization for release of health information. full name date of birth member or subscriberid individual’s _ individual’s street address c...